Ventana Medical Systems’ PATHWAY anti-c-KIT (9.7) Primary Antibody is intended for laboratory use, via light microscopy, for the qualitative detection of KIT protein in formalin-fixed, paraffin-embedded gastrointestinal stromal tumors (GISTs) using either an automated immunohistochemistry staining system or a manual assay. It is indicated as an aid in the selection of GIST within the context of the patient’s clinical history, tumor morphology, and other diagnostic tests evaluated by a qualified pathologist. It may be used after the diagnosis of GIST as an aid in the selection of GIST patients who may qualify for imatinib mesylate (Gleevec/Glivec) therapy. PATHWAY anti-c-KIT (9.7) Primary Antibody is optimized for use on a Ventana automated slide stainer and for manual application in combination with Ventana Medical Systems’ iVIEW DAB Detection Kit and accessories. The clinical interpretation of any staining, or the absence of staining, must be complemented by morphological studies and evaluation of proper controls. Evaluation must be made by a qualified pathologist within the context of the patient’s clinical history and other diagnostic tests. Prescription only. The Role of KIT Gene Mutations in the Development of GISTs:
In their landmark 1998 publication, Dr. Hirota and his colleagues established not only that GISTs express KIT, but that KIT gene mutations are present in these tumors. Furthermore, they showed that the resulting mutant KIT isoforms demonstrate kinase activity in the absence of stem cell factor, the natural ligand for KIT. These observations have been confirmed by a growing number of groups and it is now established that KIT mutations are present in >85% of GISTs. The majority of mutations occurs in exon 11 (65-70% of GISTs) and includes a wide range of deletions, insertions, point mutations, or combinations thereof. An insertion/reduplicat
ion of six base pairs in exon 9 is found in ~15% of GISTs, almost exclusively in those arising in the small intestine. Mutations also occur in exons 13 and 17, but are much rarer. Regardless of the exon involved, KIT gene mutations in GISTs are invariably in-frame and, when cloned and expressed in vitro, have constitutive kinase activation. Moreover, phosphorylation of KIT is consistently detectable in GIST tumor extracts, supporting a direct role for KIT in intracellular signaling. Clinical Significance:
GISTs arise predominantly in the stomach (60%) and small intestine (25%), but also occur in the rectum (5%), esophagus (5%) and a variety of other locations (5%), including appendix, gallbladder, mesentery, and omentum. Affected patients range in age from the teens to the 90’s, but the majority are older and the peak is around age 60. A slight male predilection has been observed in most studies. There are no solid figures on the true incidence of GISTs, but it is estimated that ~4,500 new cases are diagnosed each year in the United States. In 1998, Drs. Seichi Hirota (Osaka University) and Lars-Gunnar Kindblom (University of Gothenburg) each independently observed that GISTS express the receptor tyrosine kinase KIT (CD117). Their observations provided a clue to the possible cell of origin for GISTs, namely the interstitial cells of Cajal (ICC). These inconspicuous, dendritic-like cells are widely distributed throughout the muscularis propria of the esophagus, stomach, small and large bowel. They play an important role in gut motility by regulating slow-wave contractions. Like GISTs, ICC express KIT and the majority are also positive for CD34. The hypothesis that GISTs are pathogenetically related to ICC in the gut wall, as proposed by both Dr. Hirota and Dr. Kindblom, is now widely accepted. Subsequent studies from a large number of different laboratories have confirmed that KIT is the single most specific marker of GISTs. Immunodetectable KIT is present on the cell surface and/or cytoplasm of GIST tumor cells in approximately 90% of cases.
Ventana Medical Systems’ PATHWAY anti-c-KIT (9.7) Primary Antibody is intended for laboratory use, via light microscopy, for the qualitative detection of KIT protein in formalin-fixed, paraffin-embedded gastrointestinal stromal tumors (GISTs) using either an automated immunohistochemistry staining system or a manual assay. It is indicated as an aid in the selection of GIST within the context of the patient’s clinical history, tumor morphology, and other diagnostic tests evaluated by a qualified pathologist. It may be used after the diagnosis of GIST as an aid in the selection of GIST patients who may qualify for imatinib mesylate (Gleevec/Glivec) therapy. PATHWAY anti-c-KIT (9.7) Primary Antibody is optimized for use on a Ventana automated slide stainer and for manual application in combination with Ventana Medical Systems’ iVIEW DAB Detection Kit and accessories. The clinical interpretation of any staining, or the absence of staining, must be complemented by morphological studies and evaluation of proper controls. Evaluation must be made by a qualified pathologist within the context of the patient’s clinical history and other diagnostic tests. Prescription only.
The Role of KIT Gene Mutations in the Development of GISTs:
In their landmark 1998 publication, Dr. Hirota and his colleagues established not only that GISTs express KIT, but that KIT gene mutations are present in these tumors. Furthermore, they showed that the resulting mutant KIT isoforms demonstrate kinase activity in the absence of stem cell factor, the natural ligand for KIT. These observations have been confirmed by a growing number of groups and it is now established that KIT mutations are present in >85% of GISTs. The majority of mutations occurs in exon 11 (65-70% of GISTs) and includes a wide range of deletions, insertions, point mutations, or combinations thereof. An insertion/reduplication of six base pairs in exon 9 is found in ~15% of GISTs, almost exclusively in those arising in the small intestine. Mutations also occur in exons 13 and 17, but are much rarer. Regardless of the exon involved, KIT gene mutations in GISTs are invariably in-frame and, when cloned and expressed in vitro, have constitutive kinase activation. Moreover, phosphorylation of KIT is consistently detectable in GIST tumor extracts, supporting a direct role for KIT in intracellular signaling.
Clinical Significance:
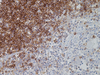
GISTs arise predominantly in the stomach (60%) and small intestine (25%), but also occur in the rectum (5%), esophagus (5%) and a variety of other locations (5%), including appendix, gallbladder, mesentery, and omentum. Affected patients range in age from the teens to the 90’s, but the majority are older and the peak is around age 60. A slight male predilection has been observed in most studies. There are no solid figures on the true incidence of GISTs, but it is estimated that ~4,500 new cases are diagnosed each year in the United States. In 1998, Drs. Seichi Hirota (Osaka University) and Lars-Gunnar Kindblom (University of Gothenburg) each independently observed that GISTS express the receptor tyrosine kinase KIT (CD117). Their observations provided a clue to the possible cell of origin for GISTs, namely the interstitial cells of Cajal (ICC). These inconspicuous, dendritic-like cells are widely distributed throughout the muscularis propria of the esophagus, stomach, small and large bowel. They play an important role in gut motility by regulating slow-wave contractions. Like GISTs, ICC express KIT and the majority are also positive for CD34. The hypothesis that GISTs are pathogenetically related to ICC in the gut wall, as proposed by both Dr. Hirota and Dr. Kindblom, is now widely accepted. Subsequent studies from a large number of different laboratories have confirmed that KIT is the single most specific marker of GISTs. Immunodetectable KIT is present on the cell surface and/or cytoplasm of GIST tumor cells in approximately 90% of cases.